



To assess the temperature variation in the cervical, middle and apical thirds of root external wall, caused by 980-nm diode laser irradiation with different parameters.
The roots of 90 canines, had their canals instrumented and were randomly distributed into 3 groups (n = 30) according to the laser potency (1.5 W, 3.0 W and 5.0 W). Each group was subdivided into 3 (n = 10) according to the frequency (CM, 100 Hz and 1000 Hz), and each subgroup divided into 2 (n = 5): dried canal or filled with distilled water. The maximum temperature values were collected by 3 thermocouples located at each third of the root external wall and recorded by digital thermometers.
The groups irradiated in the continuous mode (CM) presented the highest values (11.82 ± 5.78), regardless of the canals were dry or not, which were statistically different (p < 0.01) from those obtained with 100 Hz (6.22 ± 3.64) and 1000 Hz (6.00 ± 3.36), which presented no statistical difference between them (p > 0.01). The groups irradiated with 5.0 W presented the greatest temperature variation (12.15 ± 5.14), followed by 3.0 W (7.88 ± 3.92) and 1.5 W (4.02 ± 2.16), differing between them (p < 0.01). The cervical third of the root presented the highest temperature rises (9.68 ± 5.80), followed by the middle (7.66 ± 4.87) and apical (6.70 ± 4.23), with statistical difference among them (p < 0.01). After 30 s from the end of irradiation, all the specimens presented temperature variation lower than 10 °C.
Application of 980-nm diode laser in the root, at 1.5 W in all operating modes, and 3.0 W, in the pulsed mode, for 20 s, can safely be used in endodontic treatment, irrespective of the presence of humidity.
The root canal disinfection process begins with biomechanical preparation, by means of the mechanical action of instruments and chemical action of irrigant solutions. However, this stage does not completely eliminate the microorganisms present in long-standing infectious processes or in canals that have flattened areas and accentuated curves, which is difficult to access by instruments and irrigant solutions. Thus, microbial control also requires the use of intracanal medication, with the purpose of eliminating the microorganisms not attained by biomechanical preparation.
In spite of their antimicrobial potential, the chemical substances used in intracanal irrigation and medication are able to penetrate only up to 100 μm of the dentinal canaliculi,an insufficient depth, since the bacteria colonize the canaliculi to a depth of up to 1100 μm.
A therapeutic resource that has been researched in endodontics is laser system,a type of nonionizing light with highly concentrated energy which, in contact with live tissues, may cause a great variety of effects, depending mainly on the wavelength and the optic properties of the irradiated tissue. Among the different types of laser, Er:YAG and Nd:YAG have shown capacity for microbial reduction, smear layer removal and alter dentine surface.
Diode lasers have been gaining importance in endodontics because of being transmitted by flexible, thin fibers, which perfectly adapt to the reduced dimensions and curved from root canals, and because of presenting low acquisition and maintenance costs and being more versatile due to their compact size. In spite of their flexibility and small diameter, the fibers continue to be one of the limiting factors for use in endodontic therapy, since they irradiate the light in the direction of their long axis, which reduces their efficiency along the dentinal tubules.
Recently, a new laser of the diode family was introduced to the field of oral applications, the 980-nm diode. The wavelength of this laser gives it a high power of penetration into the tissue with a high absorption peak in melanin and hemoglobin, and low interaction with water and hydroxyapatite. This characteristic allows its energy to overtake intra and intercellular water (low coefficient of absorption) and produces a deep haemostatic and necrotic thermal effects in tissues with dark pigmentation, in comparison with Er:YAG laser.
One of the concerns about laser application inside the root canals is the conversion of light energy into caloric energy during the interaction with dentinal structures, which could generate a temperature increase in the external portion of the root and adjacent structures. Among the possible consequences of the thermal variations, damage to the cement layer is outstanding, predisposing to reabsorption of roots and periodontal ligament fibers, alveolar bone necrosis and pain. The severity of these effects is determined by the quantity of heat generated and the time that it persists in the region.
Eriksson et al described that temperatures above 56–60 °C were capable of causing protein denaturing in hard tissues. According to Eriksson and Albrektsson the temperature of 47 °C (10 °C above body temperature) for 1 min is sufficient to cause necrosis of the alveolar bone.
Ramsköld et al. also related that the increase in temperature could be deleterious to tissues adjacent to the tooth, since elevations of 10 °C, for 1 min, are still considered safe for periodontal tissue, which is less susceptible to thermal damage when compared with bone tissue, due to its high degree of vascularization.
Recently, a study conducted by Castro et al indicated that diode lasers could cause severe damage to the root surface and that some of its effects have not yet been completely determined, making it relevant to determine parameters, in vitro, which minimize thermal damage in order to enable safe and efficient use of this technology in the root canal system in vivo.
Considering the afore-mentioned facts, and due to the few reports in the literature about the use of this laser in endodontics, the aim of the present study was to assess, in vitro, the variations in temperature at the cervical, middle and apical thirds of the external root wall caused by 980-nm diode laser irradiation, at 1.5 W, 3.0 W and 5.0 W, and continuous and chopped modes with 100 Hz and 1000 Hz.
Ninety human uniradicular canines, with single straight canals, and absence of calcifications or reabsorptions were cross-sectioned in the cervical portion, close to the amelo-cement junction, using a double-faced diamond disk (KG Sorensen, Barueri, SP, Brazil), standardizing the roots at a 17 mm length.
The roots were submitted to biomechanical preparation by the Crown-Down technique, with apical stop made with a # 50 K-type file (Dentsply-Maillefer, Ballaigues, Switzerland) at 1 mm from the apex. Every time the file was changed, irrigation was performed with 2 mL of distilled and deionized water, and 10 mL for final irrigation.
After biomechanical preparation, the roots were positioned in an aluminum mold (16 mm × 16 mm × 27 mm) and had their apical portion embedded in acrylic resin. The roots were radiographed in the vestibulo-lingual direction to measure the density and thickness of the proximal walls, by means of the digital radiographic system for Windows (DIGORA; Soredex-Finndent-Orion Corporation, Helsinki, Finland).
The specimens were randomly distributed into 3 groups (n = 30) according to the laser potency (1.5 W, 3.0 W and 5.0 W) and each group subdivided into 3 (n = 10) according to the frequency (continuous mode, 100 Hz and 1000 Hz). Each subgroup was finally divided into 2 (n = 5) considering the aspect of root canal during the irradiation: completely dry or full of distilled water.
The laser used was the 980-nm diode (SIROlaser 2.2, SIRONA Dental, Bensheim, Germany), with flexible fiber optic 200 μm in diameter.
For laser application, the specimens were placed in an adjustable acrylic device, which kept them in a standardized vertical position, and allowed 3 K-type thermocouples, Chromel/Alumel to be fixed, coupled to 2 digital thermometers, one model MT-600, 2 data channels and the other MT-505, 1 data channel (MINIPA, São Paulo, Brazil), to collect the temperature at the external root walls at 15 mm, 9 mm and 3 mm above the root apex . A thermal paste (Implastec, Votorantim, Brazil) was placed at the extremities of the pairs to optimize their contact with the cement surface. The laser device was calibrated according to the manufacture's instructions before irradiation to guarantee that the settings showed on the display matched with those delivered by the fiber tip.
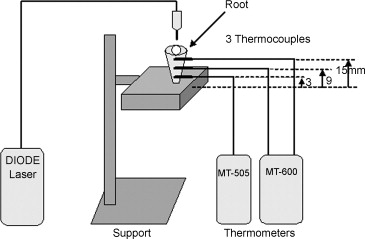
Schematic illustration of the set of appliances used (2 thermometers and the diode laser), the root fixed in a standardized support, and 3 thermocouples positioned on the cemental wall at 3 mm, 9 mm and 15 mm from the root apex.
Laser irradiation was applied for 20 s in each specimen, the fiber tip being displaced at a speed of approximately 1.5 mm/s, from the most apical part of the canal, in helicoidal movements along it, up to the cervical part and then returning to the apex. For each specimen, the back and forth movement along the canal was made only once, at all times endeavoring to keep the fiber tip in contact with the dentine wall. After each subgroup was irradiated, 2 mm were cut from the extremity of the laser fiber to start a new application.
The experiment was conducted in a room with an ambient temperature controlled at 26 °C.
After each test specimen was irradiated, one waited for the entire measuring system temperature to return to this value to start a new radiation.
The physical density and dentinal wall thickness, and temperature variation results obtained were submitted to analysis of variance (ANOVA) and Tukey tests.
The proximal root wall density and thickness values in the cervical, middle and apical thirds are expressed in . The ANOVA revealed that there was no significant difference among the studied groups (p > 0.05), indicating that the samples used in this research were similar with regard to the mentioned factors.
The root canal system disinfection process consists of reducing the microorganisms in order to enable tissue repair. The complex anatomy of root canals, however, offers opportunity and conditions for the growth, multiplication and interaction of microorganisms in pulp infections.
Currently, laser technology has been incorporated into the therapeutic arsenal in endodontics because it presents the capacity for microbial reduction in the root canal at depths of up to 1 mm in the dentinal canaliculi, a higher distance than that achieved by chemical substances, thus justifying its use in endodontic therapy.
One of the aspects that should be pointed out with regard to the methodology use concerns standardization of the dentinal wall thickness and density, since dentin and water are the main components involved in transferring the heat produced by irradiation in the root canals, as they have different heat absorption and conduction properties. Since the quantity of water present in dentine can be affected by its degree of sclerosis, determination of parameters such as density and dentinal volume available for energy absorption becomes relevant.
The temperature measurements of our study were performed in isolated root samples at room temperature, as also used by other authors. The thermal bath was not used because the contact of the thermocouples and laser tip with water during irradiation in root canal might hinder the execution of the experiment, since the temperature was measured on cervical, middle and apical third using 3 thermocouples in contact with the root surface simultaneously to the helicoidal movements with the laser tip in the interior of root canals. Besides, some authors consider that the thermal bath is less similar to the in vivo situation, due to the freely circulating water and to the large volume of cooling liquid available in the water bath.
In the present study, the application of 980-nm diode laser inside the root canal, for 20 s, at 1.5 W in all operating modes (CM, 100 Hz and 1000 Hz), and 3.0 W in chopped mode (100 Hz and 1000 Hz), did not result in temperature rises higher than 10 °C. With 3.0 W in continuous mode, and 5.0 W in all modes, there were temperature rises of over 10 °C, which makes it unfeasible to use them safely in endodontic therapy. These results can be explained because the highest potency value provided a larger quantity of light energy, which generates higher alterations in temperature. Similarly, the continuous operating mode produces uninterrupted heat, when compared with the chopped mode, which present alternating periods of energy and rest, consequently producing less tissue heating.
These results are in agreement with those described by Gutknecht et al. in their study with 810-nm diode laser, in which they concluded that application in continuous mode presented higher temperature rises in irradiated tissues in comparison with pulsed modes. However, in their study, the increase in frequency resulted in higher temperature rises, contrary to the results of the present study, which did not show difference. This divergence can be explained by the difference in the modes of production and emission of the laser system. The laser used in this study produces a continuous wave with a constant maximum value in all the operating modes. The emission in the chopped mode is achieved by means of a mechanical device, thus maintaining its peak value unchanged; whereas the laser operating mode used by Gutknecht et al. was pulsed wave, that can produce large peak of laser energy in extremely short time intervals, resulting in higher temperature values, as the frequency of the pulses rises.
Bahcall et al., when investigating the histological effect on the periapex in dogs, after irradiating the root canals with 1064 nm Nd:YAG laser (3 W/30 s), demonstrated necrosis of the periodontal ligament followed by bone reabsorption and akylosis. These results correlate positively with the temperature variations observed in the present study, in which the application of 980-nm diode laser, with the same potency value and mode of operation resulted in temperature rises above the limit recommended by the literature, with an irradiation time of 20 s. Although the studies used different types of lasers, their wavelengths are very close, which allow the interaction with dental tissues.
Another important factor in heat conduction between the canal and the periradicular tissues is the thickness of the dentinal walls, since the thicker walls make the passage of heat more difficult. Kreisler et al. demonstrated that irrespective of the heat source, the thickness of the dentin layer has a significant effect on the alteration of temperature and its subsequent histologic reactions. In the present study, the thicknesses found were, in decreasing order: 2.04 ± 0.24 mm (cervical third), followed by the middle (1.60 ± 0.18) and apical (1.17 ± 0.17), however, the highest temperature variation values were recorded in the cervical third (9.65 ± 5.77), followed by the middle (7.67 ± 4.87), and lastly, the apical (6.73 ± 4.23) third. These results are not in agreement with the findings of the mentioned authors, however, they can be explained because roots without crowns were used, which enable greater inclination of the laser fiber in the cervical region, directing the light beam more perpendicularly to the dentinal wall, and thus, achieving greater efficiency in energy delivery than in the other thirds.
Anic et al. concluded that the light beam positioned parallel to the dentine surface produced fewer morphological alterations on this surface in comparison with the more perpendicular position. In accordance with the morphology of the root canal, the greater quantity of laser energy was found in the axial direction of the irradiated beam, and less or no energy was found perpendicularly to the fiber tip, directly incident on the dentinal wall. In the present study, another factor that also justifies the higher temperature values obtained in the cervical third, was making spiral movements with the fiber tip touching the dentinal walls from the apical to the cervical and then returning to the apical region. This kinetics resulted in irradiation staying longer and continuously in the cervical third, causing higher temperature rises.
In this experiment, when root canals were irradiated with a laser, half of them were dry and the other half were full of distilled water. According to recent studies, lasers with small wavelengths, belonging to the infrared region – close to the electromagnetic spectrum, into which the diode family fits – have a low coefficient of absorption in water and hydroxyapatite, and therefore, a high transmission through them, interfering little in the temperature variations. This explanation confirms the results observed in the present study, in which there was no statistically significant difference (p < 0.01) between the groups with water (8.20 ± 4.87) and the dry groups (7.83 ± 5.38).
Considering the difficulties of experimental reproduction of the oral conditions, the great diversity in the existent laser systems, each with different and specific properties, as well as the variety of parameters that can be adopted, it becomes complex and difficult to extrapolate the results of studies that use different laser systems. However, it would appear that the investigated laser might be acceptable for endodontic application, but requires clinical evaluation to be sure.
Therefore, the results obtained in the present study open perspectives to new investigations considering the parameters that provide temperature increases within the safety limits of periapical tissues. Besides, further researches can be developed to observe the structural alterations promoted by laser irradiation on the root dentine surface, and its interferences in the bonding of filling sealers.
Under the conditions of this study, it may be concluded that the application of 980-nm diode laser in the root canal, at 1.5 W in all operating modes, and 3.0 W, in the chopped mode for 20 s, can safely be used in endodontic treatment, irrespective of the presence of humidity.